Tubal Recanalisation
Know About
Laparoscopic Tubal Recanalisation
Tubal factor is responsible in 20% of the women with infertility.
The most common predisposing factors are pelvic inflammatory disease, previous pelvic surgery, endometriosis, pelvic tuberculosis and appendicitis. The common presentations are tubo ovarian adhesions, proximal tubal block and distal tubal block or hydrosalpinx. Approximately 1% of women who undergo tubal sterilization subsequently request reversal.
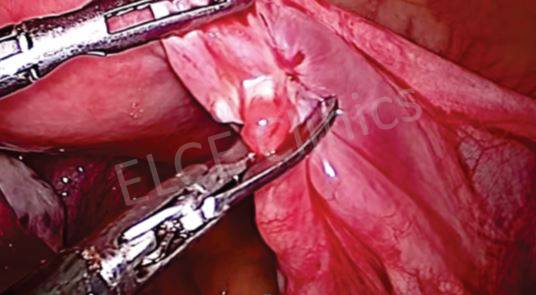
Recent improvements in laparoscopic microsurgical instruments allow tubal anastomosis to be performed by laparoscopy. Proximal tubal block is now treated by hysteroscopic cannulation.
Copyright ©2025 all rights reserved. Designed by ProPlus Logics.