Therapeutic Endoscopy
Know About
Therapeutic Endoscopy
Dr. P.S. Rajan is an advanced Therapeutic Endoscopist with extensive hands on skill in Interventional Endoscopic procedures. Some of the procedures are the following.

Banding
- Effective in controlling bleeding because of varices seen in chronic liver disease.
- Outpatient procedure – needs one or two times to completely clear varices.
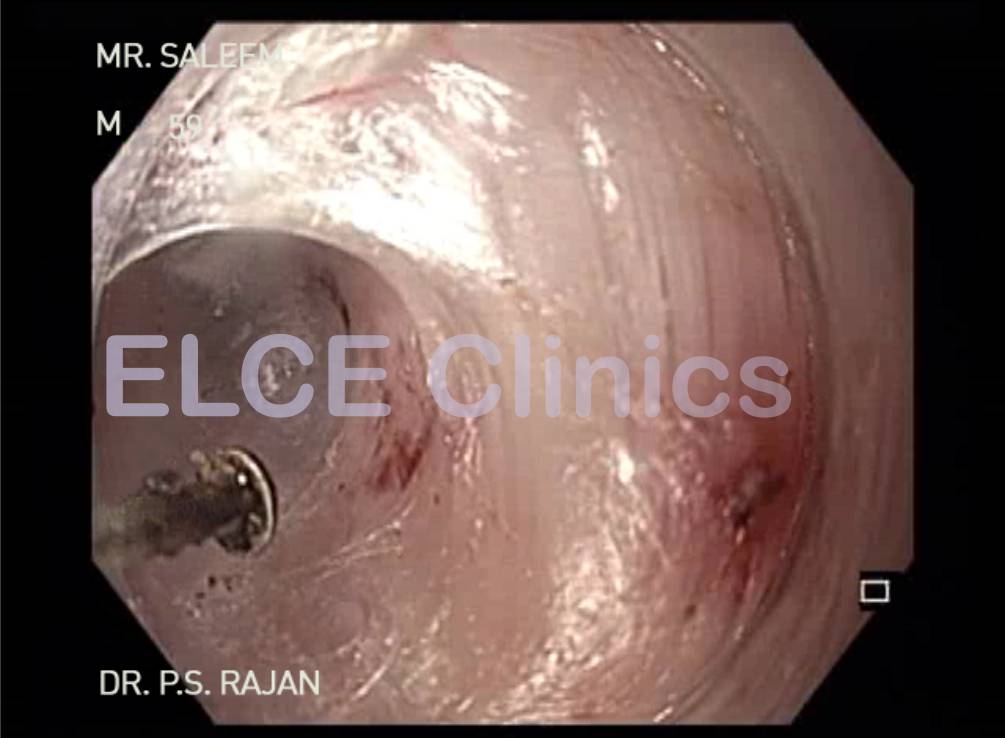
Esophageal Stricture
- To confirm with endoscopy and biopsy to R/o malignancy.
- Removable Self expanding metal stenting indicated for recurrent benign stricture, resistant to repeated balloon dilatation.
- Effective in 70–80 % of benign stricture of esophagus.
Foreign body
- Foreign body impaction in esophageal lumen by denture (or) chicken (or) Fish bone.
- If not presenting early, this can lead to abscess formation at the site of impaction.
- Flexible endoscopy is effective in retrieving such impacted foreign bodies.
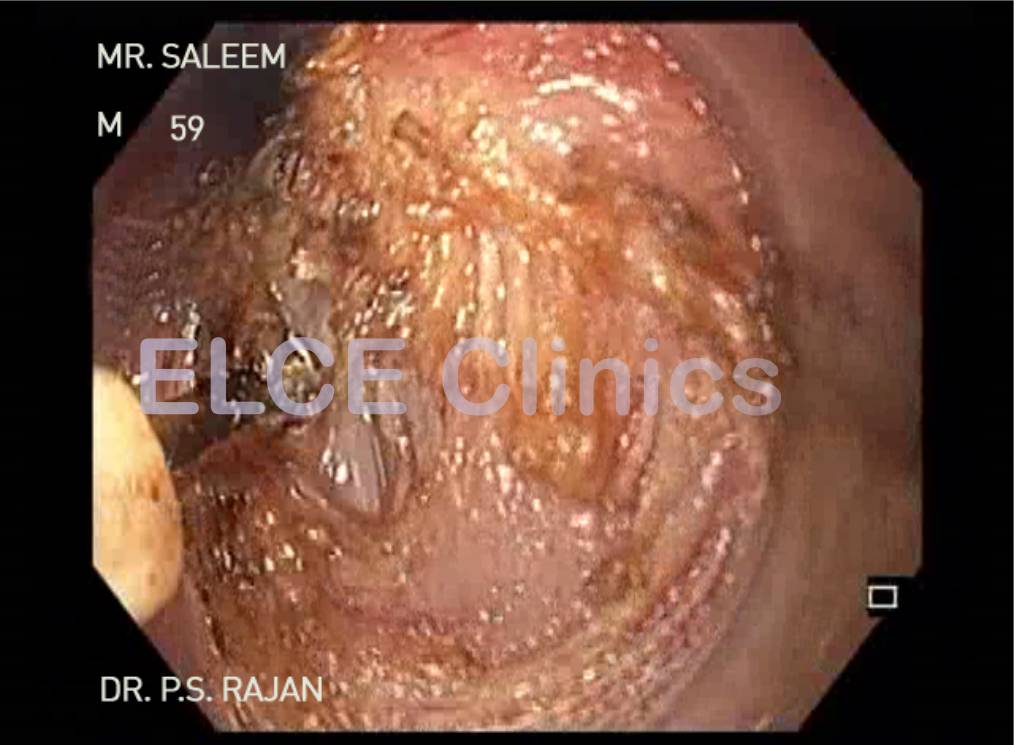
Esophageal leak
- Commonly seen after surgical procedure like esophagectomy and achalasia cardia.
- If detected early, OGD to assess the leak and deploying removable self expanding metal stent will seal the leak – stent can be removed after 3-4 months.
Therapeutic Endoscopy - ELCE clinics



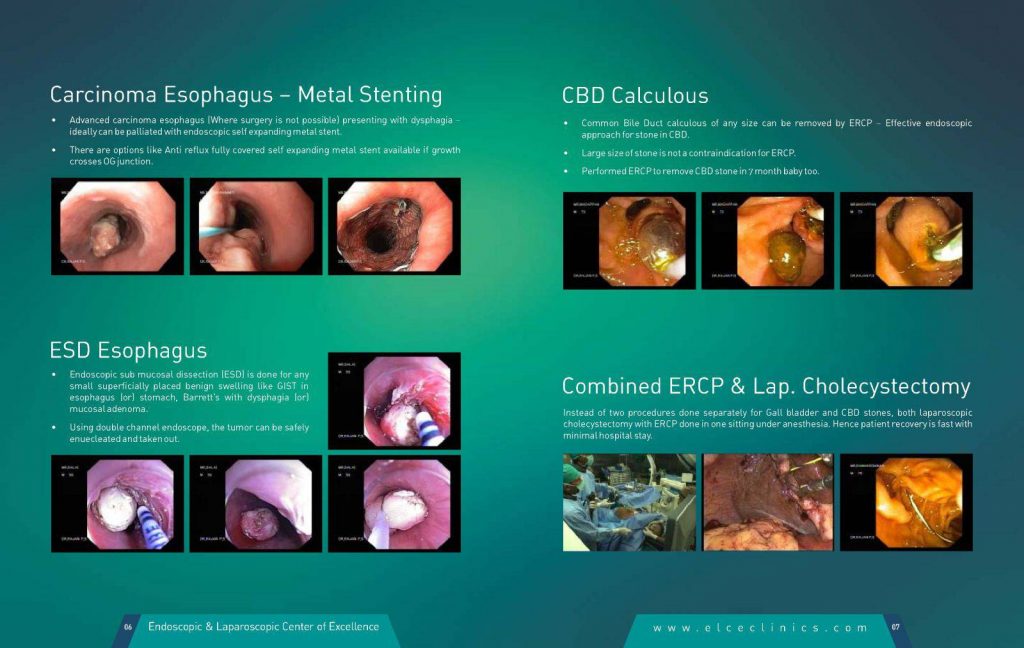
Carcinoma Esophagus – Metal Stenting
- Advanced carcinoma esophagus (Where surgery is not possible) presenting with dysphagia – ideally can be palliated with endoscopic self expanding metal stent.
- There are options like Anti reflux fully covered self expanding metal stent available if growth crosses OG junction.
ESD Esophagus
- Endoscopic sub mucosal dissection (ESD) is done for any small superficially placed benign swelling like GIST in esophagus (or) stomach, Barrett’s with dysphagia (or) mucosal adenoma.
- Using double channel endoscope, the tumor can be safely enuecleated and taken out.
CBD Calculous
- Common Bile Duct calculous of any size can be removed by ERCP – Effective endoscopic approach for stone in CBD.
- Large size of stone is not a contraindication for ERCP.
- Performed ERCP to remove CBD stone in 7 month baby too.
Combined ERCP & Lap. Cholecystectomy
- Instead of two procedures done separately for Gall bladder and CBD stones, both laparoscopic holecystectomy with ERCP done in one sitting under anesthesia. Hence patient recovery is fast with minimal hospital stay.
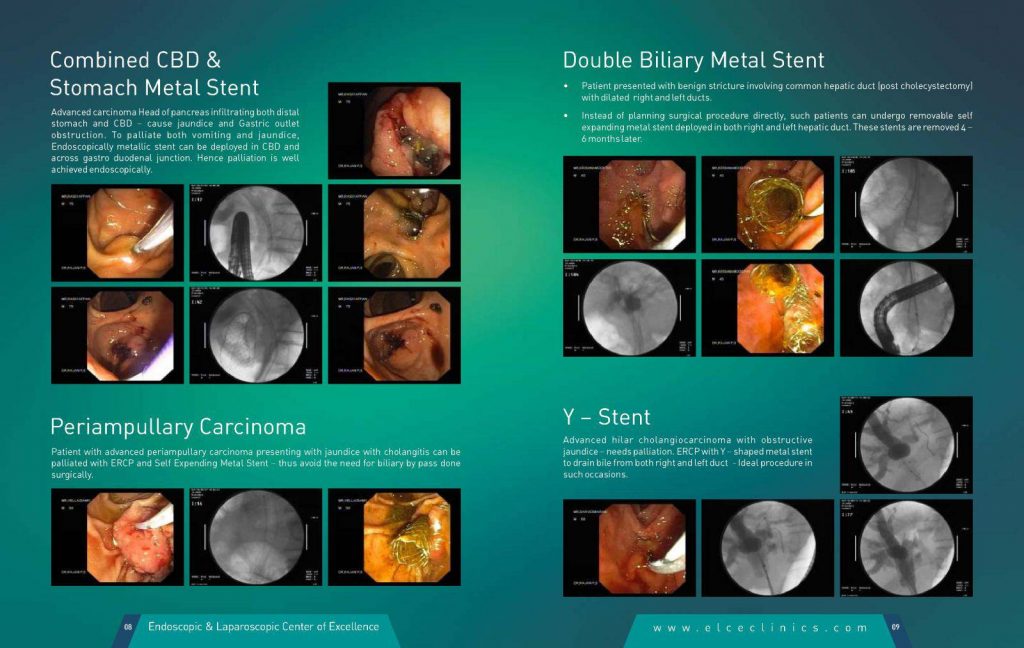
Combined CBD & Stomach Metal Stent
- Advanced carcinoma Head of pancreas infiltrating both distal stomach and CBD – cause jaundice and Gastric outlet obstruction. To palliate both vomiting and jaundice, Endoscopically metallic stent can be deployed in CBD and across gastro duodenal junction. Hence palliation is well achieved endoscopically.
Periampullary Carcinoma
- Patient with advanced periampullary carcinoma presenting with jaundice with cholangitis can be palliated with ERCP and Self Expending Metal Stent – thus avoid the need for biliary by pass done surgically.
Double Biliary Metal Stent
- Patient presented with benign stricture involving common hepatic duct (post cholecystectomy) with dilated right and left ducts.
- Instead of planning surgical procedure directly, such patients can undergo removable self expanding metal stent deployed in both right and left hepatic duct. These stents are removed 4 – 6 months later.
Y – Stent
- Advanced hilar cholangiocarcinoma with obstructive jaundice – needs palliation. ERCP with Y – shaped metal stent to drain bile from both right and left duct – Ideal procedure in such occasions.
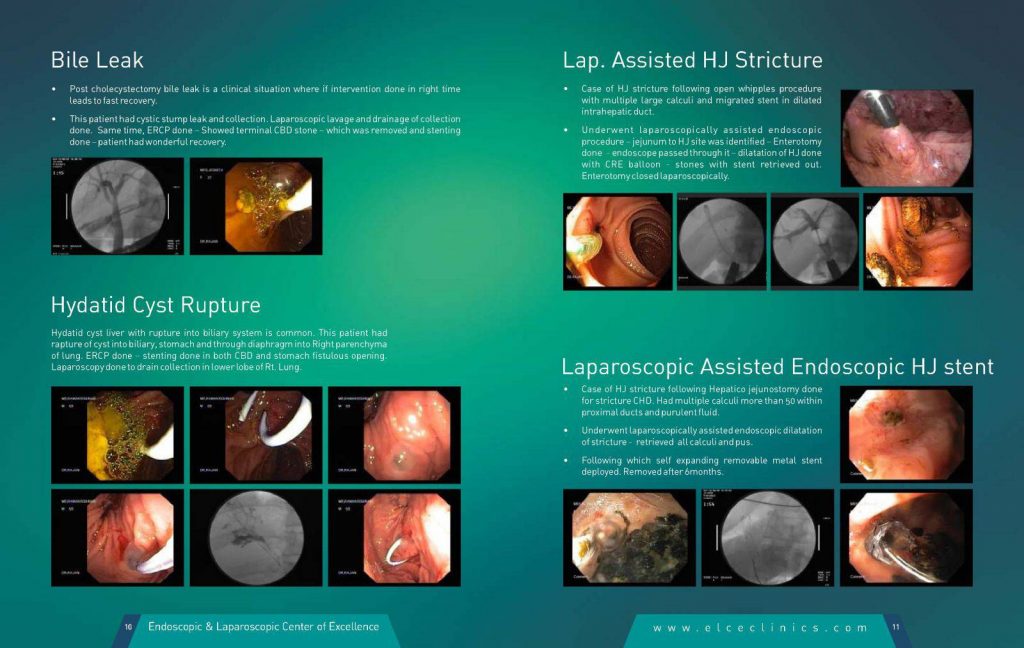
Bile Leak
- ion done in right time leads to fast recovery.
- This patient had cystic stump leak and collection. Laparoscopic lavage and drainage of collection done. Same time, ERCP done – Showed terminal CBD stone – which was removed and stenting done – patient had wonderful recovery.
Hydatid Cyst Rupture
- Hydatid cyst liver with rupture into biliary system is common. This patient had rapture of cyst into biliary, stomach and through diaphragm into Right parenchyma of lung. ERCP done – stenting done in both CBD and stomach fistulous opening. Laparoscopy done to drain collection in lower lobe of Rt. Lung.
Lap. Assisted HJ Stricture
- Case of HJ stricture following open whipples procedure with multiple large calculi and migrated stent in dilated intrahepatic duct.
- Underwent laparoscopically assisted endoscopic procedure – jejunum to HJ site was identified – Enterotomy done – endoscope passed through it – dilatation of HJ done with CRE balloon – stones with stent retrieved out. Enterotomy closed laparoscopically.
Laparoscopic Assisted Endoscopic HJ stent
- Case of HJ stricture following Hepatico jejunostomy done for stricture CHD. Had multiple calculi more than 50 within proximal ducts and purulent fluid.
- Underwent laparoscopically assisted endoscopic dilatation of stricture – retrieved all calculi and pus.
- Following which self expanding removable metal stent deployed. Removed after 6months.
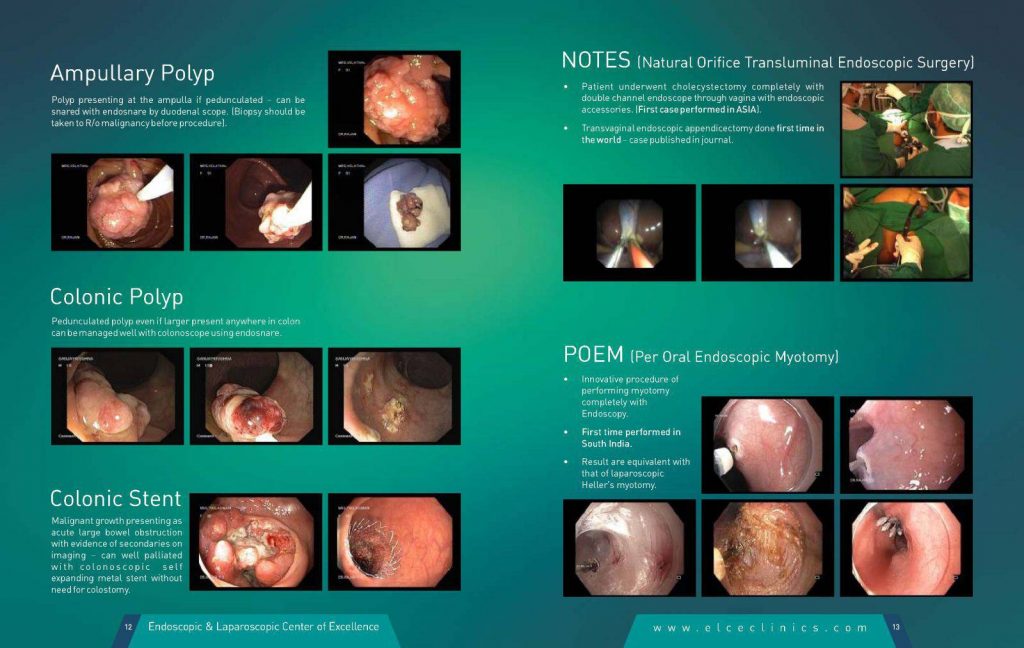
Ampullary Polyp
- Polyp presenting at the ampulla if pedunculated – can be snared with endosnare by duodenal scope. (Biopsy should be taken to R/o malignancy before procedure).
Colonic Polyp
- Pedunculated polyp even if larger present anywhere in colon can be managed well with colonoscope using endosnare.
Colonic Stent
- Malignant growth presenting as acute large bowel obstruction with evidence of secondaries on imaging – can well palliated with colonoscopic self expanding metal stent without need for colostomy.
NOTES (Natural Orifice Transluminal Endoscopic Surgery)
- Patient underwent cholecystectomy completely with double channel endoscope through vagina with endoscopic accessories. (First case performed in ASIA).
- Transvaginal endoscopic appendicectomy done first time in the world – case published in journal.
POEM (Per Oral Endoscopic Myotomy)
- Innovative procedure of performing myotomy completely with Endoscopy.
- First time performed in South India.
- Result are equivalent with that of laparoscopic Heller’s myotomy.
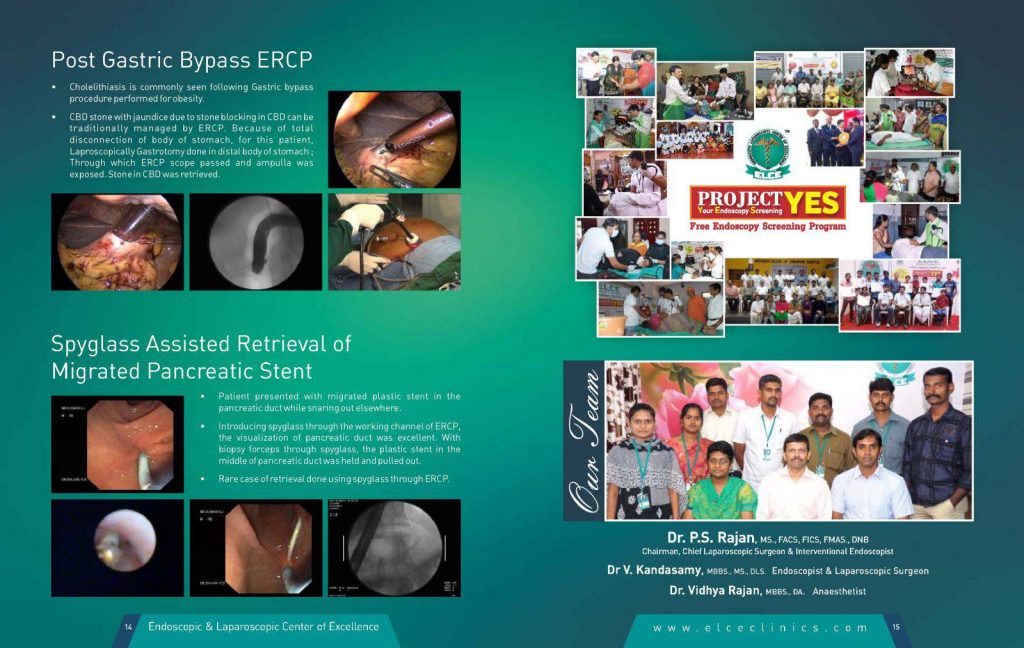
Post Gastric Bypass ERCP
- Cholelithiasis is commonly seen following Gastric bypass procedure performed for obesity.
- CBD stone with jaundice due to stone blocking in CBD can be traditionally managed by ERCP. Because of total disconnection of body of stomach, for this patient, Laproscopically Gastrotomy done in distal body of stomach ; Through which ERCP scope passed and ampulla was exposed. Stone in CBD was retrieved.
Spyglass Assisted Retrieval of Migrated Pancreatic Stent
- Patient presented with migrated plastic stent in the pancreatic duct while snaring out elsewhere.
- Introducing spyglass through the working channel of ERCP, the visualization of pancreatic duct was excellent. With biopsy forceps through spyglass, the plastic stent in the middle of pancreatic duct was held and pulled out.
- Rare case of retrieval done using spyglass through ERCP.
POEM (Per Oral Endoscopic Myotomy)
- Innovative procedure of performing myotomy completely with Endoscopy.
- First time performed in South India.
- Result are equivalent with that of laparoscopic Heller’s myotomy.
Copyright ©2025 all rights reserved. Designed by ProPlus Logics.